

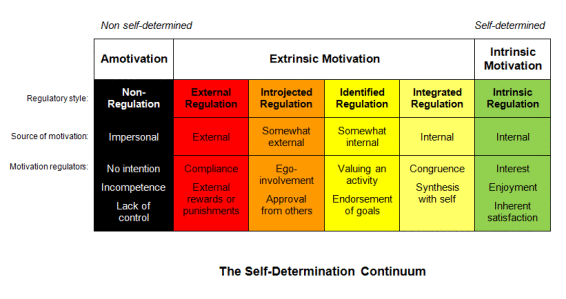
The table above provides a nice breakdown of the SDT Continuum. I’ve made it a clickable link for any of you go-getters who really want to soak it in, but for the rest of us “meat and potatoes”-types, I’ll keep it brief;
- Extrinsic motivation (EM) isn’t necessarily bad, but there are sub-types of it that are definitely less good (see: External and Introjected Regulation). These can be extremely motivating, but will likely involve negative emotions and will not withstand the test of time.
E.g. Patient A comes to you with LBP and explains that they need to get better ASAP because the pain is causing them to miss work, their employer is upset with them, and they’re losing wages and have bills to pay.
- Identified Regulation and Integrated Regulation are better versions of Extrinsic Motivation where people value the activity or have integrated it into their current values; they’re motivated because they’ve identified the activity as personally important or have integrated this activity and its outcomes to be congruent with their current values or needs
E.g. Patient B comes to you with LBP and explains that they need to get better because their pain is impeding their exercise routine and although they don’t really enjoy exercising, they know it’s important for their health (something they value)
- Intrinsic Motivation (IM) is the most powerful version of motivation in that it is linked to inherent satisfaction and enjoyment, making it the most enduring and resilient form.
E.g. Patient C comes to you with LBP and explains that they need to get better because she loves spending time hiking the local trails and hasn’t been able to do so since the pain began.
Patient A, Patient B, and Patient C are all motivated to get better, however Patient A’s motivation will last only as long as their pain does, Patient B’s motivation will persevere only as long as they continue to value their health, but Patient C’s motivation is likely to endure as it is linked to something of great inherent satisfaction or value for them.
Our goal as practitioners isn’t necessarily to have all of our patients be like Patient C, but rather it’s to help move patients along this continuum toward more self-determined forms of regulation. The question is... how?!
Well, Self Determination Theory posits that human motivation is based on the satisfaction of 3 universal needs;
Autonomy: The need to perceive our behaviours and thoughts as freely chosen
Competence: The need to perceive our behavior and interactions as effective; to believe that we can and will succeed (thank you, self-efficacy theory)
Relatedness: The need to perceive that we are connected to those around us; that we belong
The idea being that, the degree to which these needs are met when engaging in (or contemplating) a certain behaviour or activity will determine what type of motivation drives that behaviour. The more they’re met, the more self-determined the type of motivation.
So, if we apply this theory to Physical Therapy, how can you create an environment for your patients that supports these needs, thereby facilitating more self-determined forms of motivation and all the good things that come with it? Well, if we look at some of the literature from the exercise psychology world, we can pull out a few good suggestions.

To Foster Autonomy
