
I love what these Tendon savants have going on. They make a point to bridge the gap between research and the clinical setting and offer clear pragmatic principles and clinical reasoning processes to help us with these challenging patients. See what I’m talking about and check out some of their blogs and podcasts here: (
La Trobe Tendinopathy Blog,
Peter Malliaras's Blog,
BJSM Podcast)
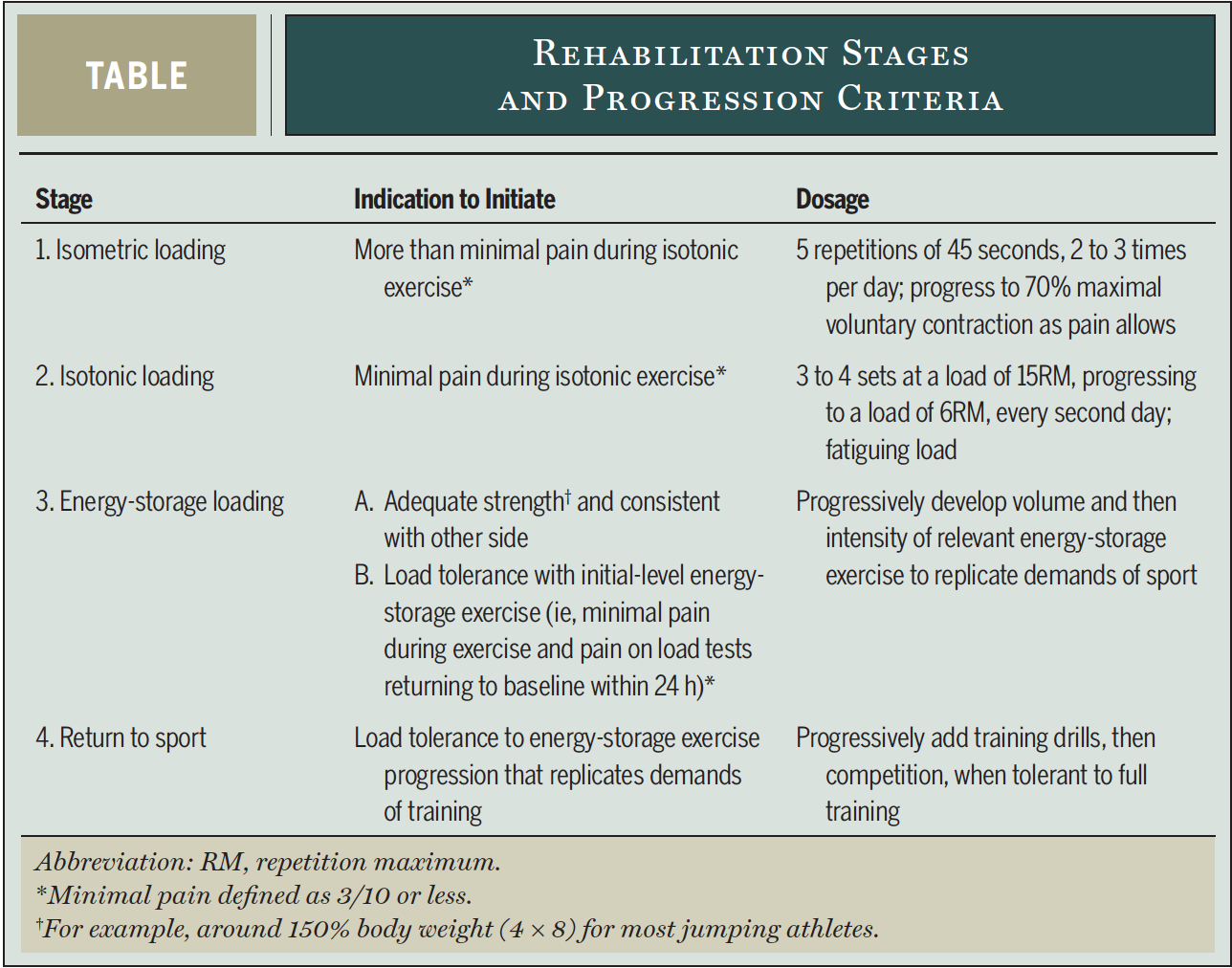
In this blog, we’ll get into lower limb tendinopathy. Starting with a bit of background info, and then exploring the 4-stage treatment process that can give a framework for your treatment decisions and goals.
You can’t fake and bake tendinopathy. There’s just too much variability in presentation for there to be a certain exercise or a certain protocol that will work for everyone. What we do have is a guiding principle: RESTORE FUNCTION! I know that sounds nebulous… but that’s why we made a blog about it.
After you've decided that it is in fact a Tendinopathy, and you have an idea of the variables and risk factors that paint the clinical picture, go on to educate and address expectations early:
- "The focus of rehab is on developing the tendon's ability to tolerate loads and on strengthening the muscles in the area."
- “Once a tendon, always a tendon”. The part of the tendon that is degenerative stays degenerative (I'd use a different word than degenerative... try wonky). "What we're going to do is treat the doughnut (the healthy tissue around the wonky tissue) not the hole."
- "This will likely take a while." Get buy in for prolonged rehab program. Treating a highly irritable tendon can take months to get back to full function.

1) Some pain is acceptable during and after exercise (ideally <3/10), but symptoms should resolve reasonably quickly after exercise and not progressively worsen over the course of the loading program, as monitored by the 24hr Load Response:
- At the same time every day, the patient does a load tolerance test and compares each day’s pain score to his or her baseline pain score.
- If the pain is higher than his baseline score, it means the previous day's load has NOT been tolerated. This will red light or green light progressing.
2) Heavy Slow Resistance (HSR) exercises are better than eccentric exercises. Pain and function will improve with both exercise strategies, but patient satisfaction (and therefore real life compliance) is much better in the HSR exercisers.
RefGoal: reduce pain and facilitate loading that would otherwise be made difficult due to pain. This has an added benefit of getting buy-in from your patient.
- Use isometrics in isolation during this stage.
- This stage may last 3+ weeks in patients with high irritability.
- Regional strength exercises are appropriate but be sure to spare the painful muscle-tendon unit. Target your regional isotonic exercises at anti-gravity muscles distal to the site of pain.
- 5 reps of 45-second isometric mid-range loading
- Intensity: 70% max voluntary contraction (they should not be able to last longer than 45 seconds with this weight).
- Frequency: 2-3 times a day with 2 minutes of rest between each rep.
This has been shown to:
- Reduce tendon pain for the next 45 minutes.
- Reduce motor cortex inhibition of the quadriceps
- Progress by increasing resistance as quickly as tolerated.
Note:
- Too little resistance won’t work.
- An immediate reduction in pain is a great prognostic factor and will assist in confirming the diagnosis.
- Progressing too quickly won’t work.

- Goal: restore muscle bulk and strength.
- Progress to this when it can be performed with minimal pain (<3/10).
- Stay within the bounds of the 24 hr load response test.
- Use a Heavy Slow Resistance strategy. Which is exactly what it sounds like.
- Load in positions that don’t put the tendon in compression.
- In addition to standard double-leg multi-joint exercises, ensure that you include unilateral exercises and exercises that isolate the specific muscle-tendinous unit.
- Dose: 3-4 sets at 15-rep max progressing to 6 rep max (heavy load is important and needed to get tendon adaptation).
- Stage 1 isometric exercises are to be included on the off days to manage pain.
- Progress to this stage when you have good strength (compared to the opposite side), and minimal pain during these exercises (<3/10 and clear 24-hr load response test)
- Individualize these exercises based on the sport/activities they want to get back to. The rate of tendon loading is key here.
- Examples: jumping and landing, acceleration, deceleration, and cutting. (choose the ones relevant to their sport)
- Start at a level that your patient can tolerate, and progress by increasing first volume and then intensity to the point of sport simulation.
- Can take several weeks to months.
- This is the usually the most provocative phase, so start slow with loading sessions every three days initially.
- Use the 24 hr load tolerance test to guide increasing or decreasing loads.
- Use stage 1 exercises to manage pain.
Try this schedule:
Day 1: Stage 3 energy storage loading exercises.
Day 2: Stage 1 isometrics.
Day 3: Stage 2 isotonic Loading.Repeat then take a day off.
- Start this when the athlete has simulated the sport demands with stage 3 energy storage exercises.
- Replace stage 3 exercises with a gradual return to sport.
- Keep the same 3 day schedule.Return to competition is commenced when full training is tolerated without symptom provocation.
- For the first year of return to sport, perform no more than 3 training or competition sessions a week that involve energy-storage exercises.
From Malliaras and colleagues’ 2015 Clinical Commentary in JOSPT (
Ref)
- Perform stage 2 (isotonic) exercises twice per week.
- Perform stage 1 (isometric) exercises as needed for pain control (eg pre competition)
- Continue strengthen the region focusing on weak muscle groups.
- Unrealistic rehabilitation time frames
- Inaccurate beliefs and expectations about pain
- Failure to identify central sensitization
- Over reliance on passive treatments
- Not addressing isolated muscle deficits
- Failure to address kinetic-chain deficits
- Not addressing biomechanics

- Address expectations early, get buy in, and commitment to the treatment plan.
- Progress deliberately and systematically through the 4 stages with daily feedback from the 24 load tolerance test.
- Restore confidence, promote self-efficacy, and nudge them to have positive expectations.
- Don't rely on passive treatments. For tendinopathy, they're a load of crap.
